



Amyotrophic Lateral Sclerosis (ALS) Panel
Summary and Pricing 
Test Method
Exome Sequencing with CNV Detection| Test Code | Test Copy Genes | Panel CPT Code | Gene CPT Codes Copy CPT Code | Base Price | |
|---|---|---|---|---|---|
| 10155 | Genes x (29) | 81479 | 81179(x1), 81404(x1), 81405(x1), 81406(x3), 81407(x1), 81479(x51) | $990 | Order Options and Pricing |
Pricing Comments
The C9orf72 hexanucleotide repeat expansion will be performed first as this is the most common cause of ALS. If C9orf72 testing is negative then the ALS sequencing panel and ATXN2 repeat expansion testing will be performed. Results for the C9orf72, ATXN2, and sequencing panel tests will be reported separately. Concurrent testing is available upon request. C9ORF72 and ATXN2 repeat expansions are available separately if needed.
We are happy to accommodate requests for testing single genes in this panel or a subset of these genes. The price will remain the list price. If desired, free reflex testing to remaining genes on panel is available. Alternatively, a single gene or subset of genes can also be ordered via our Custom Panel tool.
An additional 25% charge will be applied to STAT orders. STAT orders are prioritized throughout the testing process.
Click here for costs to reflex to whole PGxome (if original test is on PGxome Sequencing platform).
Click here for costs to reflex to whole PGnome (if original test is on PGnome Sequencing platform).
Turnaround Time
C9orf72 assays completed within 2 weeks on average for standard orders. Reflexive panels are completed within an additional 4 weeks on average for standard orders.
Please note: Once the testing process begins, an Estimated Report Date (ERD) range will be displayed in the portal. This is the most accurate prediction of when your report will be complete and may differ from the average TAT published on our website. About 85% of our tests will be reported within or before the ERD range. We will notify you of significant delays or holds which will impact the ERD. Learn more about turnaround times here.
Targeted Testing
For ordering sequencing of targeted known variants, go to our Targeted Variants page.
Clinical Features and Genetics
Clinical Features
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease characterized by motor neuron impairment in the cortex, brain stem, and spinal cord (Hardiman et al. 2017. PubMed ID: 28980624). The dysfunction and loss of these neurons results in rapid progressive muscle weakness, atrophy and ultimately paralysis of limb, bulbar and respiratory muscles. About 50% of patients also develop cognitive and behavioral impairment and another 13% develop frontotemporal dementia (van Es et al. 2017. PubMed ID: 28552366). The mean age of symptom onset is 55 years of age for familial cases and 65 years of age for sporadic cases; most cases begin between 40 and 70 years of age. The annual incidence of ALS is 2-3 per 100,000 (van Es et al. 2017. PubMed ID: 28552366; Brown and Al-Chalabi. 2017. PubMed ID: 28700839; Siddique and Siddique. 2019. PubMed ID: 20301623).
ALS has a heterogeneous clinical presentation with variable disease progression and age related penetrance. Classic ALS presentation occurs in ~70% of all cases. About two-thirds of classic cases present with spinal neurodegenerative primarily affecting lower leg and upper arm motor neurons and one-third of classic cases present with bulbar involvement resulting in dysartheria and/or dysphagia. 5-15% of all ALS cases present with bulbar or spinal neurodegeneration and dementia; 5% present with bulbar only features without spreading to other regions; and 10% present with only lower motor neuron involvement (van Es et al. 2017. PubMed ID: 28552366; Siddique and Siddique. 2019. PubMed ID: 20301623; Brown and Al-Chalabi. 2017. PubMed ID: 28700839).
Genetics
About 10% of ALS cases are familial (FALS) with the majority being inherited in an autosomal dominant manner with age-dependent penetrance. In rare cases, the disease is transmitted in an autosomal recessive or dominant X-linked pattern. About 90% of ALS cases are sporadic (SALS) with no known affected relatives; however, ~8% of these have positive genetic findings (Zou et al. 2017. PubMed ID: 28057713).
The C9orf72, SOD1, FUS, and TARDBP gene account for 35%, 15%, 3% and 4% of European FALS cases respectively. In Asian FALS patients, pathogenic variants in the C9orf72, SOD1, FUS, TARDBP genes account for 2%, 30%, 6% and 1.5% cases (Zou et al. 2017. PubMed ID: 28057713). The SOD1 p.Asp91Ala variant (also referred to as p.Asp90Ala in literature) is a known founder variant within the Scandinavian population and has been shown to result in autosomal recessive ALS (Andersen et al. 1995. PubMed ID: 7647793). Pathogenic variants in the UBQLN2 gene are associated with X-linked ALS (Brown and Al-Chalabi. 2017. PubMed ID: 28700839; Siddique and Siddique. 2019. PubMed ID: 20301623). Autosomal dominant forms of ALS include pathogenic variants in the ANG, ANXA11, ARHGEF28, CFAP410 (C21orf2), C9orf72, CHCHD10, CHMP2B, DCTN1, ERBB4, FIG4, FUS, HNRNPA1, HNRNPA2B1, KIF5A, MATR3, MOBP, NEFH, NEK1, OPTN, PFN1, SETX, SQSTM1, TAF15, TARDBP, TBK1, TUBA4A, UNC13A, VAPB, and VCP genes.
An expansion of a GGGGCC hexanucleotide repeat in a non-coding region of the C9orf72 gene is the most common inherited cause of ALS (Renton et al. 2011. PubMed ID: 21944779; DeJesus-Hernandez et al. 2011. PubMed ID: 21944778). Alleles with less than 25 repeats are usually considered normal (Majounie et al. 2012. PubMed ID: 22406228; van der Zee et al. 2013. PubMed ID: 23111906). Alleles with more than 30 repeats are considered pathogenic (Renton et al. 2011. PubMed ID: 21944779). This expanded repeat accounts for up to 40% of FALS cases and 7% of SALS cases (Byrne et al. 2012. PubMed ID: 22305801). The GGGGCC hexanucleotide repeat expansion was reported in patients with ALS, ALS-FTD or FTD (Siddique and Siddique. 2019. PubMed ID: 20301623).
ATXN2 expansions of the exon 1 poly glutamine track ranging from 29-32 CAG repeats have also been associated with an increased risk for development of ALS (Van Damme et al. 2011. PubMed ID: 21562247). While expansions >32 repeats are typically associated with Spinocerebellar Ataxia 2 (SCA2), patients with ALS and with >32 repeats have been reported (Sproviero et al. 2017. PubMed ID: 28017481; Ross et al. 2011. PubMed ID: 21610160). For example, ALS was reported in a family with one affected individual being homozygous for 33 repeats and a second affected individual being compound heterozygous for 31 and 33 repeats (Van Damme et al. 2011. PubMed ID: 21562247).
See individual gene summaries for information about molecular biology of gene products and spectra of pathogenic variants.
Clinical Sensitivity - Sequencing with CNV PGxome
Genetic causes are identified in 40-60% of FALS cases and 3-8% of SALS cases. Pathogenic variants in the C9orf72 (40%), SOD1 (1-50%), FUS (1-5%), and TARDBP (1-5%) genes account for the majority of familial cases (Zou et al. 2017. PubMed ID: 28057713). Pathogenic variants in the ANG, SQSTM1, PFN1, UBQLN2, OPTN, VCP, and VAPB genes account for less <1% of FALS cases. Clinical sensitivity for the ANXA11, ARHGEF28, CFAP410, CHCHD10, CHMP2B, DCTN1, ERBB4, FIG4, HNRNPA1, HNRNPA2B1, KIF5A, MATR3, MOBP, NEFH, NEK1, OPTN, SETX, TAF15, TBK1, TUBA4A, and UNC13A genes is currently unknown due to the limited number of cases reported to date, but is expected to be low (Robberecht and Philips. 2013. PubMed ID: 23463272; Brown and Al-Chalabi. 2017. PubMed ID: 28700839). The majority of genes in this panel have no or very few large deletions/duplications.
Testing Strategy
The C9orf72 hexanucleotide repeat expansion will be performed first as this is the most common cause of ALS. If C9orf72 testing is negative then the ALS sequencing panel and ATXN2 repeat expansion testing will be performed. Results for the C9orf72, ATXN2, and sequencing panel tests will be reported separately. Concurrent testing is available upon request.
Both the C9orf72 and ATXN2 repeat expansion tests each utilize four unique gene specific assays: (1) a repeat primed PCR assay with the locus specific primer 5’ (upstream) of the repeat region (2) a repeat primed PCR assay with the locus specific primer 3’ (downstream) of the repeat region and two unique fluorescent fragment length assays. C9orf72 and ATXN2 are not included in the sequencing panel.
The sequencing panel typically provides 99.0% coverage of all coding exons of the genes listed plus 10 bases of flanking noncoding DNA in all available transcripts along with other non-coding regions in which pathogenic variants have been identified at PreventionGenetics or reported elsewhere. We define coverage as ≥20X NGS reads or Sanger sequencing. PGnome panels typically provide slightly increased coverage over the PGxome equivalent. PGnome sequencing panels have the added benefit of additional analysis and reporting of deep intronic regions (where applicable).
Dependent on the sequencing backbone selected for this testing, discounted reflex testing to any other similar backbone-based test is available (i.e., PGxome panel to whole PGxome; PGnome panel to whole PGnome).
Indications for Test
Candidates for testing typically present with upper and lower motor neuron impairment with other diagnoses excluded via imaging and neurophysiological examinations. Diagnosis can be difficult as sites of symptom onset and disease progression can be variable. Other screening tools used for ALS include the ALS-Brief Cognitive Assessement (ALS-BCA), the ALS Cognitive Behavioral Scressn (ALS-CBS) and the Edinburgh Cognitive and Behavioral ALS Screen (ECAS) (van Es et al. 2017. PubMed ID: 28552366).
Candidates for testing typically present with upper and lower motor neuron impairment with other diagnoses excluded via imaging and neurophysiological examinations. Diagnosis can be difficult as sites of symptom onset and disease progression can be variable. Other screening tools used for ALS include the ALS-Brief Cognitive Assessement (ALS-BCA), the ALS Cognitive Behavioral Scressn (ALS-CBS) and the Edinburgh Cognitive and Behavioral ALS Screen (ECAS) (van Es et al. 2017. PubMed ID: 28552366).
Genes
| Official Gene Symbol | OMIM ID |
|---|---|
| ALS2 | 606352 |
| ANXA11 | 602572 |
| ATXN2 | 601517 |
| C9orf72 | 614260 |
| CHCHD10 | 615903 |
| CHMP2B | 609512 |
| DCTN1 | 601143 |
| DNAJC7 | 601964 |
| FUS | 137070 |
| GLE1 | 603371 |
| KIF5A | 602821 |
| MATR3 | 164015 |
| NEK1 | 604588 |
| OPTN | 602432 |
| PFN1 | 176610 |
| SETX | 608465 |
| SIGMAR1 | 601978 |
| SOD1 | 147450 |
| SPG11 | 610844 |
| SPTLC1 | 605712 |
| SPTLC2 | 605713 |
| SQSTM1 | 601530 |
| TARDBP | 605078 |
| TBK1 | 604834 |
| TUBA4A | 191110 |
| UBQLN2 | 300264 |
| UNC13A | 609894 |
| VAPB | 605704 |
| VCP | 601023 |
| Inheritance | Abbreviation |
|---|---|
| Autosomal Dominant | AD |
| Autosomal Recessive | AR |
| X-Linked | XL |
| Mitochondrial | MT |
Diseases
Related Tests
Citations
- Andersen et al. 1995. PubMed ID: 7647793
- Brown and Al-Chalabi. 2017. PubMed ID: 28700839
- Byrne et al. 2012. PubMed ID: 22305801
- DeJesus-Hernadez et al. 2011. PubMed ID: 21944778
- Hardiman et al. 2017. PubMed ID: 28980624
- Majounie et al. 2012. PubMed ID: 22406228
- Renton et al. 2011. PubMed ID: 21944779
- Robberecht and Philips. 2013. PubMed ID: 23463272
- Ross et al. 2011. PubMed ID: 21610160
- Siddique and Siddique. 2019. PubMed ID: 20301623
- Sproviero et al. 2017. PubMed ID: 28017481
- Van Damme et al. 2011. PubMed ID: 21562247
- van der Zee et al. 2013. PubMed ID: 23111906
- van Es et al. 2017. PubMed ID: 28552366
- Zou et al. 2017. PubMed ID: 28057713
Ordering/Specimens
Ordering Options
We offer several options when ordering sequencing tests. For more information on these options, see our Ordering Instructions page. To view available options, click on the Order Options button within the test description.
myPrevent - Online Ordering
- The test can be added to your online orders in the Summary and Pricing section.
- Once the test has been added log in to myPrevent to fill out an online requisition form.
- PGnome sequencing panels can be ordered via the myPrevent portal only at this time.
Requisition Form
- A completed requisition form must accompany all specimens.
- Billing information along with specimen and shipping instructions are within the requisition form.
- All testing must be ordered by a qualified healthcare provider.
For Requisition Forms, visit our Forms page
If ordering a Duo or Trio test, the proband and all comparator samples are required to initiate testing. If we do not receive all required samples for the test ordered within 21 days, we will convert the order to the most effective testing strategy with the samples available. Prior authorization and/or billing in place may be impacted by a change in test code.
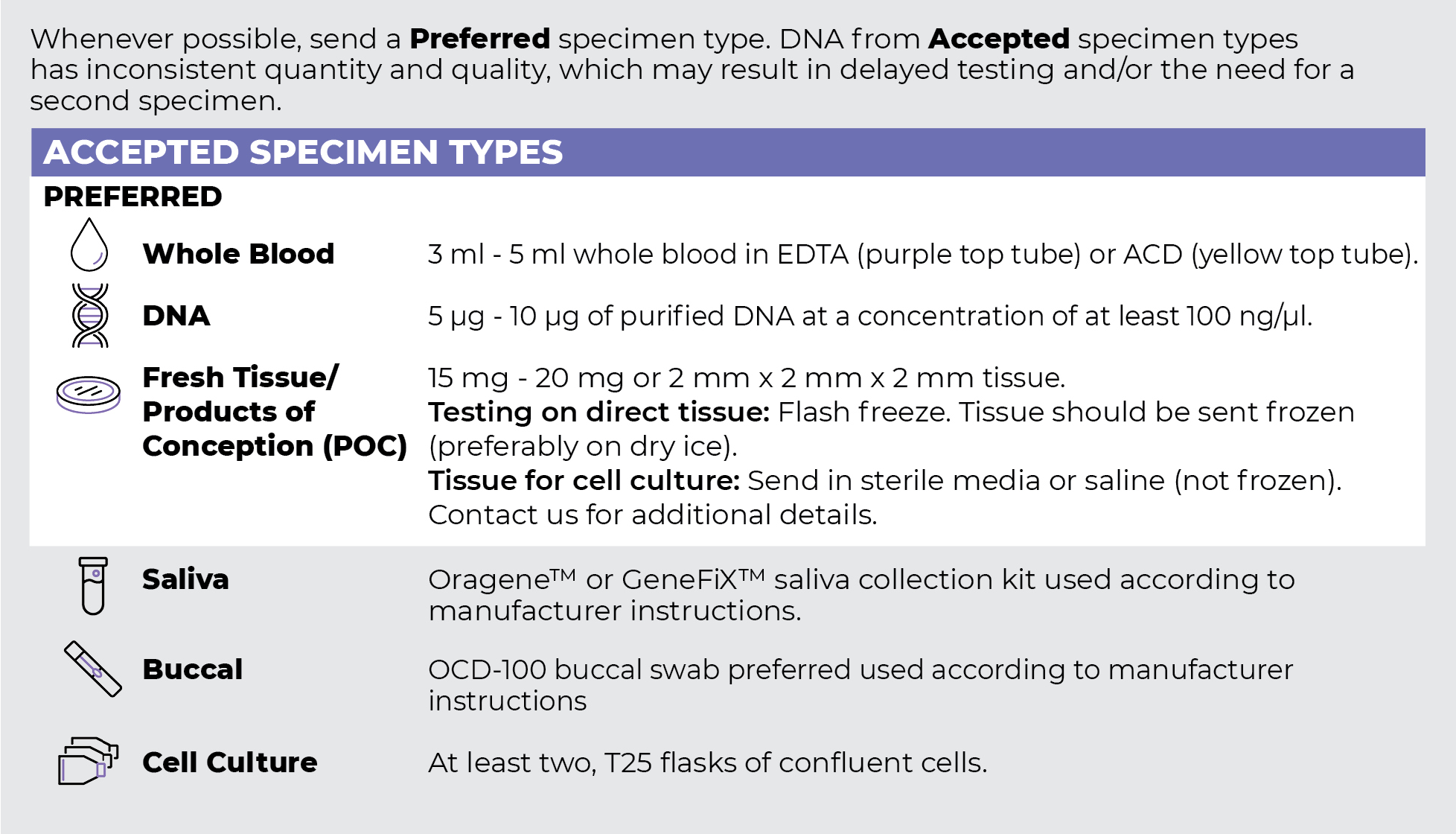
Specimen Types
Specimen Requirements and Shipping Details
PGxome (Exome) Sequencing Panel
PGnome (Genome) Sequencing Panel

ORDER OPTIONS
View Ordering Instructions1) Select Test Type
2) Select Additional Test Options
No Additional Test Options are available for this test.